How to turn occupational thermography into a protocol, not an isolated image.
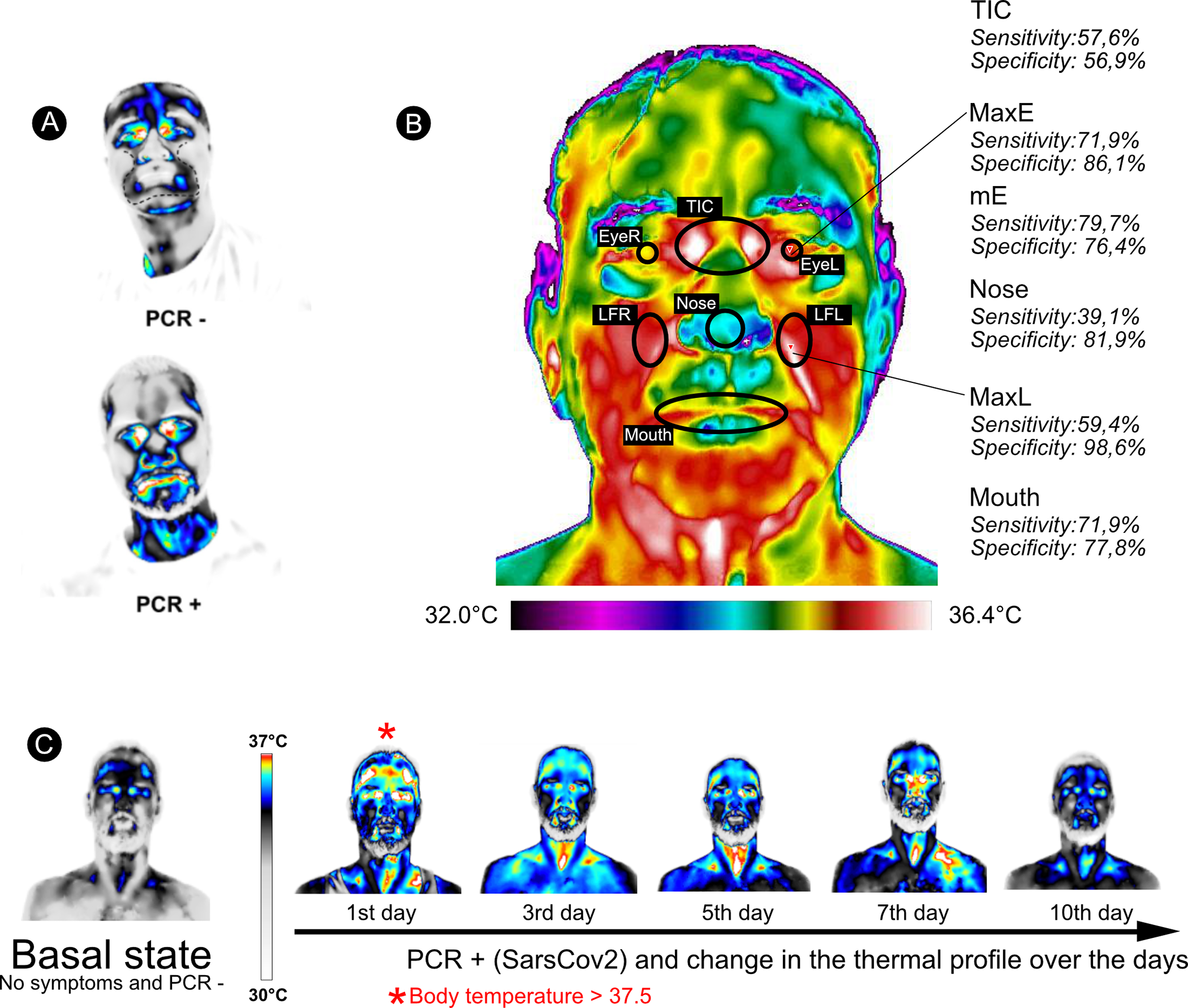
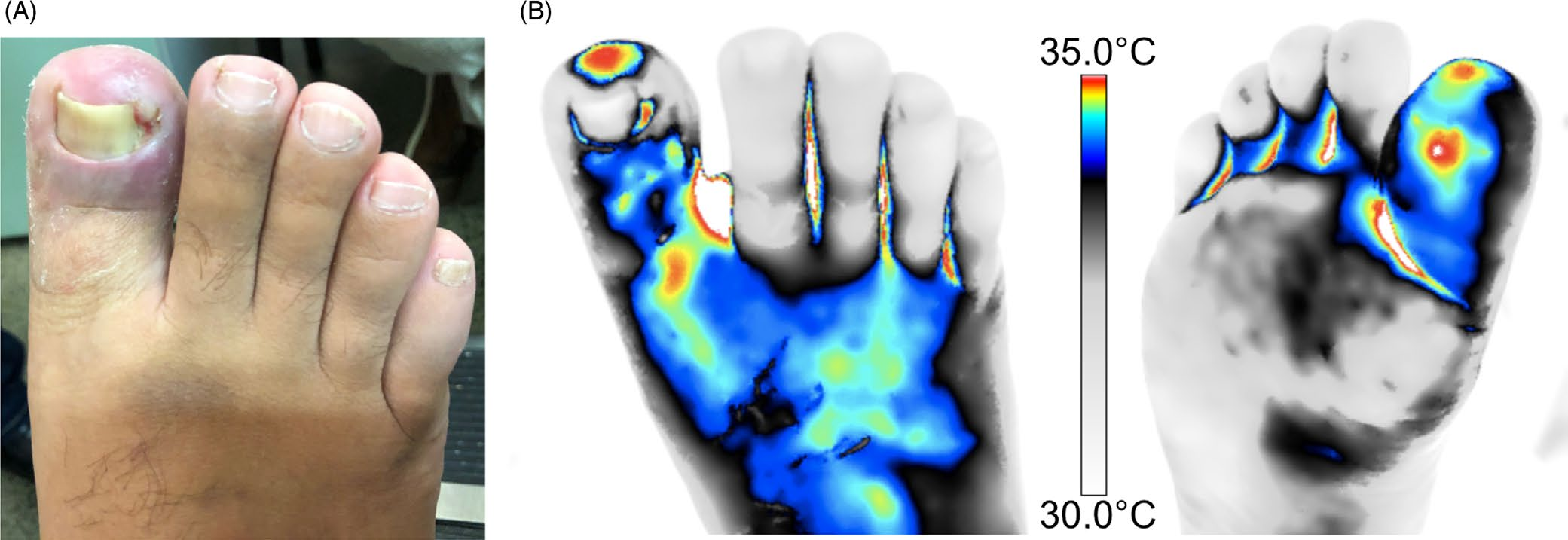
In the study by Ribeiro and Giacomini, thermography is treated as functional data: a way to observe the body thermal response when there is technical control, a clinical question, and comparison with other findings.
The starting point is concrete. Work-related musculoskeletal injuries and disorders remain major occupational health challenges. Often, the worker feels pain, fatigue, or loss of function before a structural change is evident. The review positions IRT as a complementary functional marker within a more complete occupational assessment.
Ribeiro J. A. S.; Giacomini L. A.
Exploration of Musculoskeletal Diseases. 2026;4:1007122.
DOI 10.37349/emd.2026.1007122