In a Bothrops snakebite, persistent fever may raise a difficult question: is there active infection, or is there an extensive inflammatory response sustained by the venom? The report follows this bedside question and shows how infrared thermography can add a functional layer to clinical follow-up.

The question that organizes the case
The article describes a young man from a riverside community in Oriximiná, Pará, seen about four hours after being bitten on the right leg by a snake of the genus Bothrops. The case was classified as a moderate snakebite and treated with antivenom, analgesia, wound care, and prolonged hospital follow-up.
During hospitalization, the lesion evolved with local necrosis and the patient maintained febrile episodes. Laboratory and microbiological investigation did not identify a detectable infectious focus. In this setting, fever could no longer be read only as a sign of probable infection and required an integrated reading of local and systemic inflammation.
Severe pain, edema, and bruising at the bite site. Antivenom was administered after classification as a moderate Bothrops snakebite.
Appearance of local necrosis, exudate, and persistent axillary hyperthermia, with prophylactic antibiotic therapy and wound care.
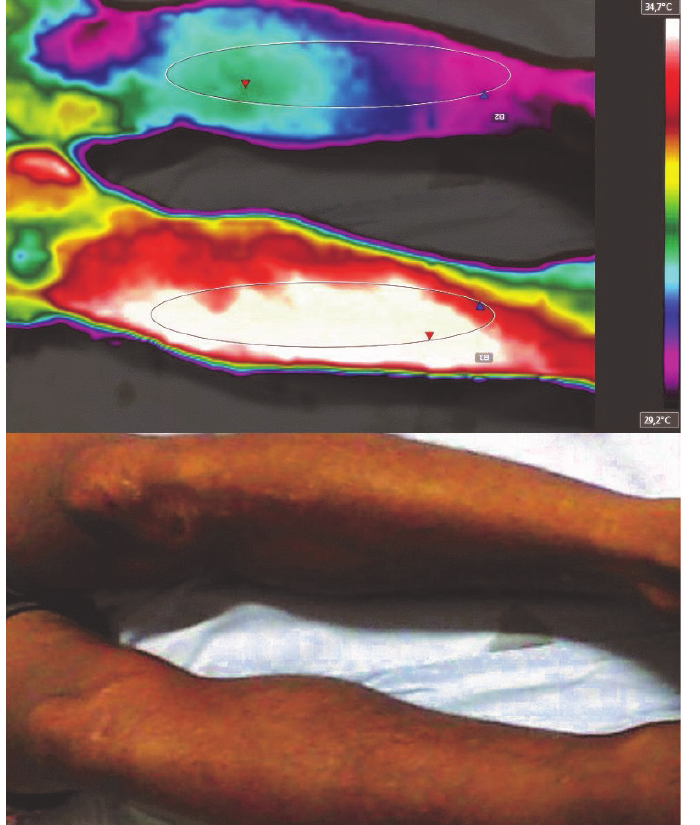
After regular anti-inflammatory and antipyretic medication was suspended, the fever curve became more evident and the first thermograms were obtained.
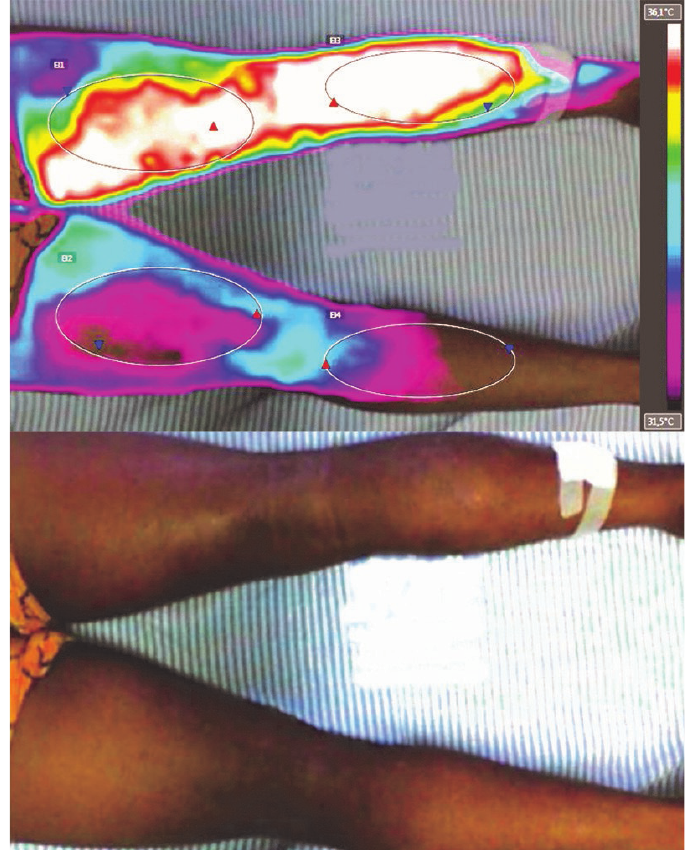
The posterior thermogram showed inflammatory extension in the lower limb, while infection tests remained negative.
In Bothrops snakebites, antibiotics may be necessary when infection is established. The challenge is not to automatically equate every persistent fever with infection, especially when venom biology can also sustain pain, necrosis, inflammatory activation, microvascular changes, and mediator release capable of modulating body temperature.
What thermography added
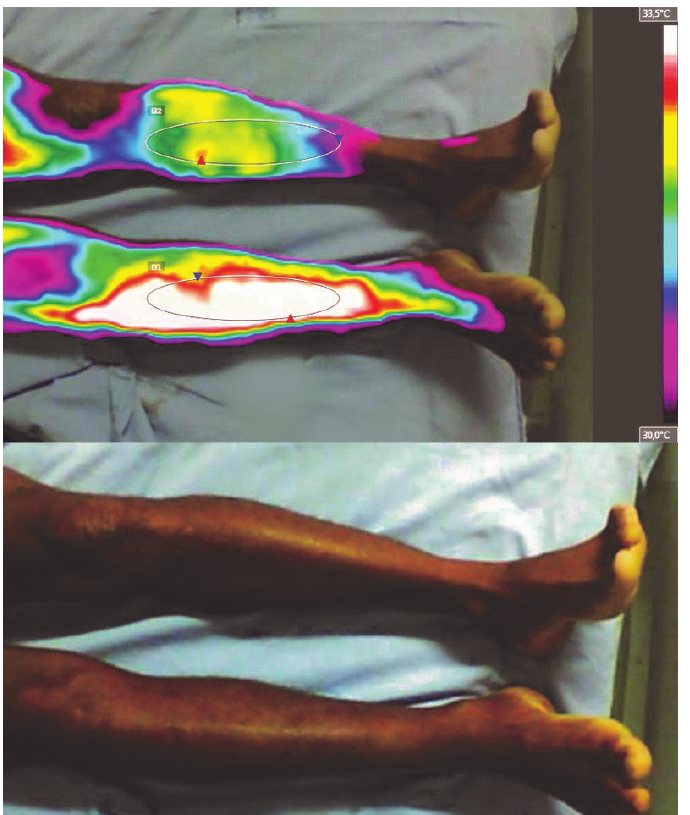
Thermography did not determine the diagnosis in isolation. It helped visualize the functional extent of the inflammatory process. By comparing regions of interest between the affected limb and the contralateral limb, the authors observed marked thermal differences that followed the clinical evolution.
The fever curve as part of the story
The study reports 24 axillary temperature measurements during hospitalization, with a mean of 37.84 °C, standard deviation of 0.67 °C, and a range from 36.6 °C to 39.2 °C. The curve helps show that the febrile phenomenon was not isolated: it accompanied the clinical process and required interpretation alongside tests, physical examination, and local evolution.
Inflammation is not a local detail
Bothrops venom is described in the literature as proteolytic, procoagulant, paradoxically hemorrhagic, and pro-inflammatory. This combination helps explain why the local lesion can be extensive, painful, and persistent, with repercussions that cannot be reduced to the appearance of the wound.
Thermal imaging makes this extent more visible because it follows the distribution of heat on the surface. Instead of looking only at one point of the wound, the method allows observation of topography, asymmetry, and regions of interest compared with the opposite limb.
Follow the thermal extent of inflammation, compare sides, document evolution, and enrich the discussion between infectious fever and inflammatory fever when the rest of the clinical picture points in that direction.
Physical examination, cultures, blood count, C-reactive protein, renal function, coagulation, vascular assessment, wound care, and individualized medical decision-making.
Thermography does not turn fever into a diagnosis. It helps visualize the thermal physiology that accompanies the lesion.
Why this post matters for medical thermology
The case shows a coherent application of thermography: not as a striking image, but as a functional follow-up tool. The clinical question already existed; the camera added a way to observe the extent and thermal variation of the inflammatory process over days.
This is the kind of use that brings medical thermology closer to translational practice. Thermal data does not need to compete with laboratory tests or anatomical methods. Its role is different: to show functional heat distribution, within protocol, in dialogue with clinical care.
Main reference
Ribeiro JAS, Gomes G, Brioschi ML, Barbosa SMM, Teixeira MJ. Inflammation and fever after Bothrops snakebite: a brief clinical-epidemiological review through case report and infrared thermography follow-up. Pan American Journal of Medical Thermology. 2019;6:87-93.
Commentary published by the Termodiagnose Journal. Scientific authorship of the original study: João Alberto de Souza Ribeiro and collaborators.